How can we offer obstetrics and gynaecology residents high-quality surgical training at a time when the number of “simple surgeries” is decreasing due to an increase in complex recruitments in expert centres, when the time devoted to them is being reduced due to pressure to optimise the number of patients operated on in the operating theatre, and when the number of obstetrics and gynaecology residents is increasing?
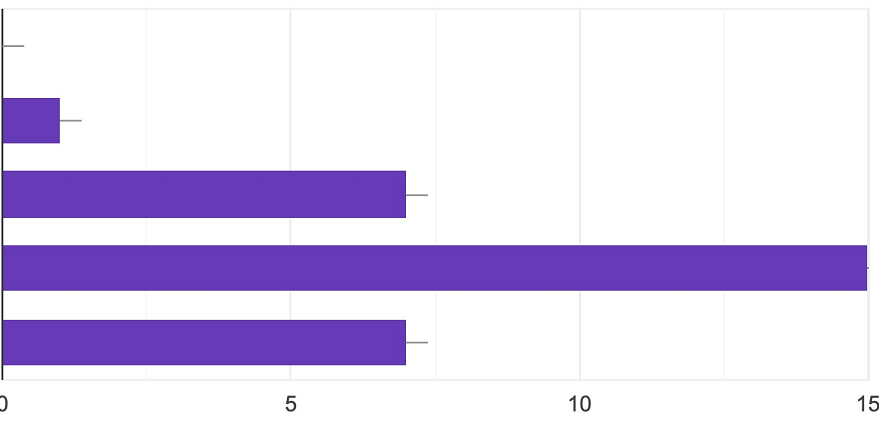
Do you think surgical videos can contribute to your training?
From top to bottom:
– I don’t know
– No
– Yes, in a minor way compared to other teaching modalities
– Yes, on a par with other teaching modalities
– Yes, in a major way and could supplant the rest
The aim of this study was to evaluate how the surgical training of interns could be improved by the use of surgical videos. There were two parts to the study: the first consisted of a survey of interns studying for the residency in Gynaecology-Obstetrics in the Ile de France region, while the second assessed the potential benefits of watching surgical videos “with support” in terms of surgical preparation.
Materials and methods
A questionnaire was submitted to Gynaecology-Obstetrics residents in the Ile de France region from various hospitals. The questionnaire was in Google Forms format and consisted of 9 multiple-response questions which included the current residency semester, the residents’ use of videos to learn about surgery and expectations of surgical videos during their training.
A cohort of obstetrics gynaecology residents from Tenon Hospital were then invited to watch videos of procedures that they should be able to perform independently at the start of their post-internship training. Each resident was given an individual assessment session. Before watching the videos for the first time, they were asked to answer a questionnaire to assess how far they had progressed in their training and how confident they were in their ability to perform the procedure independently. They then watched the videos on their own and had to write down the various surgical steps and the operating technique required to perform the operation successfully. Then, a senior surgeon (Dr Yohann Dabi) watched the same video with them, explaining in detail each of the procedures performed, identifying the different anatomical structures involved and the relationships between organs: this was ‘accompanied’ viewing. He also used an anatomy book to review the essential anatomical references for the operation. He then asked them to evaluate the possible benefit of this session. The responses were qualitative due to the small number of residents involved (4);
Results
What are the expectations of obstetrics and gynaecology residents in terms of surgical videos?
Thirty residents completed the Google Forms questionnaire, the majority of whom were in their final year of residency between the 8th and 10th semesters (24/30, 80%).
To the question “Did you receive any ‘surgical’ training on how to perform the operations during your residency?”, only 16% answered in the affirmative. On the other hand, 60% said no and that they had received “on-the-job” training by watching/helping/assisting with the surgeries in question. Finally, 30% answered no and had used videos of surgeries for educational purposes.
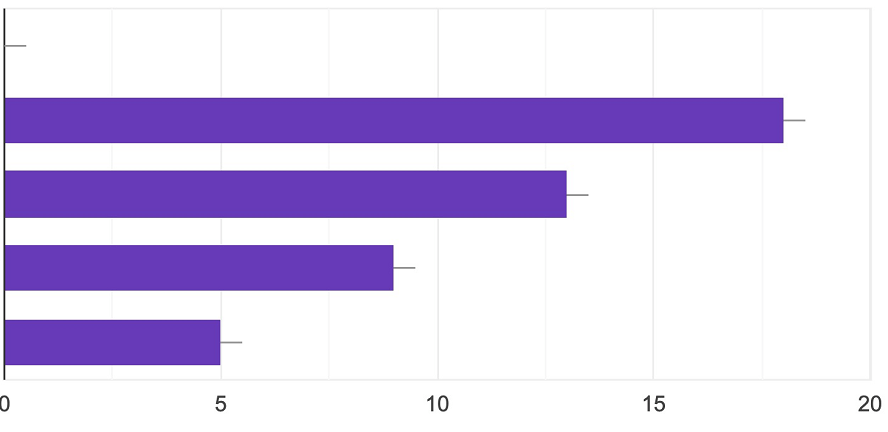
Did you receive any “surgical” training on how to carry out the operations during your residency?
From top to bottom:
– I don’t know
– No, I learned “on the job” by watching procedures
– No, but I received courses within the various departments
– No, I learned on my own by watching videos
– Yes
Half of the residents questioned felt that the use of surgical videos could contribute equally to their surgical training with the theoretical courses already given, and almost one intern in 4 thought that these videos could supplant the theoretical courses.
The residents felt that surgical videos could contribute to their training by improving their knowledge of key times (96%), anatomy (83%) and do’s and don’ts (86%). In half the cases, they were already watching videos on their own at least once a month. In these cases, the videos mainly concerned complex or laparoscopic/robotic surgery (66% and 56% respectively). Finally, one out of every two residents stated that they could not easily find quality videos for laparoscopic/robotic surgery, and this rate was even 90% for open surgery (laparotomies or vulvovaginal surgery) (Future 4).
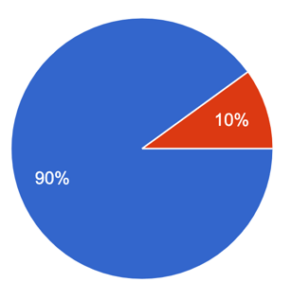
“Find quality videos for “open” surgery (including vulva-vaginal surgery) easily ” Red:Yes, Blue:No.
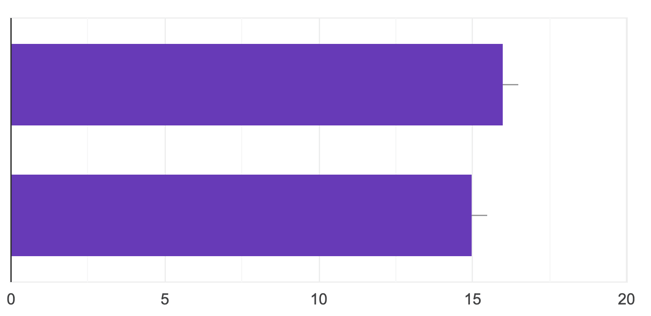
“How easy is it to find quality laparoscopic / robotic surgery videos?” Top:Yes, Bottom:No.
Contribution of “accompanied” viewing of surgical videos
The table below summarises the progress made by the interns in their training and their self-assessment before the session of their ability to carry out the procedure.
|
|
Resident 1 |
Resident 2 |
Resident 3 |
Resident 4 |
|
How many times have you performed this procedure yourself? |
10 – 20 times |
< 3 times |
Jamais |
3 – 10 times |
|
Do you think you know the key surgical times? |
Completely |
Completely |
Partially |
Completely |
|
Do you think you have mastered this procedure? (Between 1 “not at all” and 10 “perfectly”) |
6 |
6 |
5 |
4 |
|
Would you feel capable of carrying out this procedure alone (with the help of another resident, for example) ? (Between 1 “not at all” and 10 “perfectly”) |
7 |
4 |
3 |
5 |
After watching the video, the interns wrote down the various stages of the operation. Resident 3 felt that it helped him to understand the anatomical relationships, while Resident 4 felt that it helped him to “realise that certain important steps are not well understood”. Resident 1 thought it was “a good exercise” and Resident 2 learned nothing in particular.
The accompanied viewing exercise then lasted around 1.5 hours per resident.
To the question ” what did you think of the accompanied viewing ” compared to viewing alone, the responses were as follows :
Resident 1 : accompanied viewing ” allows you to review surgical times, anatomy, learn to recognise the exposure required for the procedure and how to get help, understand the reaction to adopt in the event of difficulty “, more effectively than on your own.
Resident 2 : ” It’s above all the commentary that brings real benefit to the video. Anatomy, understanding of the surgical strategy and understanding of the operating sequence (order of key times) are better understood “. She felt more comfortable about performing the surgery after the session.
Resident 3 : ” Awareness of the importance of anatomical spaces and the relationships between structures / Clarification of surgical times / Taking the time whereas on the video certain gestures are not explained and so we can’t see that they are being performed “.
Resident 4 : ” Going over the operative times in more detail, allows us to review the anatomy “
The residents evaluated were all in favour of repeating the experience and were satisfied with it. They all thought that regular similar sessions could greatly benefit their training.
Conclusion
The teaching profession must reinvent itself in order to offer the new generation of future surgeons a range of training adapted to their expectations and relevant to their generational characteristics. Surgical videos can contribute to their practical training, and it is up to senior surgeons to provide them with the quality support that they cannot easily find on the platforms currently available. Lastly, watching videos together would be time smartly invested by teachers to prepare residents as effectively as possible for the realities of surgical procedures.
Article written by Camille Mimoun, from the work of Yohann Dabi.
Read more
Surgical Video Summarization: Multifarious Uses, Summarization Process and Ad-Hoc Coordination
While surgical videos are valuable support material for activities around surgery, their summarization demands great amounts of time from surgeons, limiting the production of videos. Through fieldwork, we show current practices around surgical videos. First, we...

ResoMeds: a social network sharing videos
Case reports enrich medical knowledge and training, and improve practice [1-4]. However, their publication is often limited in existing journals [5]. We aim to highlight the importance of creating a platform for physician exchange to promote peer learning, case...
Videos improve knowledge retention of surgical anatomy
In otolaryngology, a new publication shows that an educational video improves anatomy learning and knowledge retention in the long term. This study conducted by the ENT team at Necker-Enfants Malades, APHP (Université Paris Cité) and led by Pr François Simon shows the...
Surgical videos: using the most efficient medium. AGOF’s associative experience
In 2010, the French National Authority for Health (HAS) issued the famous slogan for apprentice surgeons: "Never perform surgery on a patient for the first time" (1). It is sometimes difficult for a young surgeon to accept that he or she has not received sufficient...